Policy Statement on Alternate-Level of Care (ALC) Governance
New Brunswick Medical Society Position
Too many patients are admitted to New Brunswick hospitals under alternate level of care (ALC) circumstances. These patients are not receiving the care they need and those patients would be better served in a longer term/non acute care setting.
The N.B. Medical Society recognizes the efforts the Government of New Brunswick has made to implement the larger systemic recommendations of the Seniors’ Advocate, including efforts to transform the governance of the system, improve accountability, grow the workforce, streamline the patient assessment process and better utilize existing special care homes that have open beds.
As these systemic changes will take a significant amount of time to impact the system, we need to build a bridge that will provide agency to health professionals and civil servants to make unnecessary hospital admissions a last resort – instead of the safety net. Any other approach will continue to put acute care patients at risk in our hospitals.
NBMS Recommends:
- That government prioritize the implementation of the recommendations contained in the October 2025 Update by the New Brunswick Seniors’ Advocate with a particular focus on the introduction of a new Long Term Care Act.
- That, as a transition measure per the Advocate’s recommendation, a protocol be created where any admission resulting in a new ALC patient will require a review and signoff by a designated senior official at Social Development certifying that they have ascertained that the patient being admitted to hospital could not be reasonably cared for at home, in a special care home or in a community setting – even with exceptions being made to existing support programs.
- That this review must certify that all reasonable alternatives, including enhanced home care or community-based options, have been explored and documented. This review should include the input of the older adult, their family or supportive decision-maker. Dedicated funding should be made available to support temporary exceptions, through innovative community based or home care interventions, while individuals wait for LTC placement.
- That the Department of Social Development undertake a province wide, coordinated evaluation of all special care home and long-term care assets within the next six months to fully activate available capacity. This evaluation should provide reviewers a verified, up to date count of licensed special care home beds, with distinctions between beds that are vacant and available, vacant but closed due to staffing, and unavailable due to infrastructure or regulatory constraints.
Background
The Canadian Institute for Health Information (CIHI) defines alternate level of care (ALC) as instances when a patient is occupying a bed in a facility and does not require the intensity of resources or services provided in that care setting.[1]
Prevalence of Alternate Level of Care
A 2025 Canadian Journal of Health Technologies Study with Canada’s Drug Agency (CADTH and CDA-AMC) national Evidence Assessment determined that nationally 6.2% of hospitalizations and 17% of hospital days (range: 6.8–26.1%) involve ALC.[2]
New Brunswick fares significantly worse when compared nationally at 8.3% of hospitalizations in 2024-2025 and 32.4% of patient days in alternate level of care.[3]
These numbers can be further examined by health zone where we see ALC hospitalizations more common in northern New Brunswick.
Alternate Level of Care (ALC) hospitalizations – Percentage[4]
(Percentage of patients designated as Alternate Level of Care (ALC) out of all patients hospitalized: acute, chronic, and rehabilitation levels of care.)
| Category | Geography or group | 2024-2025 | 2023-2024 | 2022-2023 |
| Province | New Brunswick | 8.3 | 8.5 | 8.1 |
| Health zones | Zone 1 – Moncton and South-East Area | 7.6 | 8.2 | 7.4 |
| Health zones | Zone 2 – Fundy Shore and Saint John Area | 7.5 | 7.1 | 7.4 |
| Health zones | Zone 3 – Fredericton and River Valley Area | 6.6 | 6.6 | 5.7 |
| Health zones | Zone 4 – Madawaska and North-West Area | 6.4 | 6.9 | 6.4 |
| Health zones | Zone 5 – Restigouche Area | 13.1 | 10.9 | 11.9 |
| Health zones | Zone 6 – Bathurst and Acadian Peninsula Area | 14.9 | 15.8 | 13.1 |
| Health zones | Zone 7 – Miramichi Area | 9.8 | 11.1 | 12.9 |
The measure above indicates the total days where patients were designated as being on the ALC service as a proportion of the total patient days for the hospital. This measure may help hospital administrators monitor the length of stay (LOS) in ALC service and collaborate with other sectors of the health care system to improve the ALC patient flow.
Patient days in Alternate Level of Care (ALC) – Percentage[5]
(The proportion of days a patient was assigned to the alternate level of care (ALC) patient service.)
| Category | Geography or group | 2024-2025 | 2023-2024 | 2022-2023 |
| Province | New Brunswick | 32.4 | 32.9 | 34 |
| Health zones | Zone 1 – Moncton and South-East Area | 26.7 | 28.6 | 29.3 |
| Health zones | Zone 1 – Moncton and South-East Area – Horizon | n/a | 27.2 | n/a |
| Health zones | Zone 1 – Moncton and South-East Area – Vitalité | n/a | 30.2 | n/a |
| Health zones | Zone 2 – Fundy Shore and Saint John Area | 35.7 | 34.1 | 35.5 |
| Health zones | Zone 3 – Fredericton and River Valley Area | 26.3 | 26.6 | 25.2 |
| Health zones | Zone 4 – Madawaska and North-West Area | 21.3 | 25.2 | 29.5 |
| Health zones | Zone 5 – Restigouche Area | 38.3 | 34.5 | 45.1 |
| Health zones | Zone 6 – Bathurst and Acadian Peninsula Area | 55.7 | 58 | 55.7 |
| Health zones | Zone 7 – Miramichi Area | 31.3 | 35.1 | 33.6 |
Availability of Long-Term Care Beds
When one looks outside hospitals to gauge the availability of long-term care beds, we find that New Brunswick (28.8) fares reasonably well when compared to the national average at 29 LTC beds per 1,000 population age 65 and older.
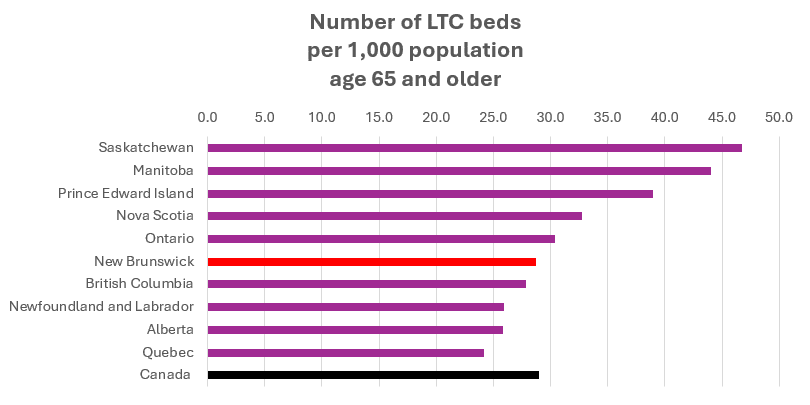
The previous chart illustrates the number of long-term care beds per 1,000 seniors (65+), CIHI (2021). Provinces are ordered from highest to lowest capacity. CIHI notes that “comparisons should be interpreted with caution due to different delivery models.”[7]
Analysis
The twin factors of ALC hospitalization and extended patient days combined with the lack of availability of long-term beds, have significant impacts at the hospital level. Specifically, ALC hospitalization continues to place enormous pressure on Emergency Departments throughout New Brunswick.
Legislation
New Brunswick Regulation 85-187 under the Nursing Homes Act, describes alternative level of care patients as:
9.04(1) A prospective resident who has been discharged from a hospital facility operated by a regional health authority as defined in the Regional Health Authorities Act but who remains in the hospital facility as an alternative level of care patient shall accept the first offer of a placement at a nursing home that offers services in the official language of choice of the prospective resident, if the nursing home:
- was selected by the prospective resident in the request, as a regular placement, or
- is 100 km or less from the residence of the prospective resident, as an interim placement.
In August of 2025 the Government of New Brunswick made changes to the Nursing Homes Act as well as the Regulation. These changes included giving the Minister of Social Development authority to override the standard nursing home waitlist for up to 120 days. The previous “critical state” admission category was eliminated and an expanded priority protocol where both hospital ALC patients and at-risk individuals in the community can be prioritized.
The triggers for “fast-track” placement under Section 9.05(1.2) of Regulation 85-187 are:
- Hospital occupancy exceeds 95%, and
- At least 25% of those beds are occupied by ALC patients (patients waiting for long-term care).
These changes allow the province to accelerate LTC placements during high-pressure periods, freeing up acute-care beds and reducing hospital congestion.
Patient Care Outcomes
Unnecessary and lengthy hospital stays for ALC patients can have a negative impact on patient outcomes over time. Hospitals are designed to provide acute care – not nursing home care; keeping an ALC patient in a hospital setting where they may not receive the type of care and services they would receive in a nursing home, may lead to cumulative negative effects over time. The New Brunswick Seniors Advocate notes in his Report on the Long-Term Care System in New Brunswick that “the longer a vulnerable adult remains in a hospital setting as an ALC patient the greater the risk of functional decline, delirium, falls, and infections, all while incurring disproportionate healthcare costs.”[8]
CIHI also states that “there is growing concern that providing ALC services in an acute care hospital is not optimum for patients who are ready to be discharged but must remain in hospital until they can be discharged to an appropriate setting. Long length of stay (LOS) for patients in ALC service can have a negative impact on the efficiency and resource use of hospitals; an example is long waits in the emergency department pending the availability of an inpatient bed.”[9]
CIHI also notes the “availability of out-of-hospital supporting health services (such as home care and long-term residential care) is often a significant factor in the delay to discharge, resulting in longer LOS in ALC service.”[10]
Further Considerations
Demographics
The demographic profile of New Brunswick is aging rapidly. New Brunswick has one of the oldest populations in Canada and this challenge will continue to worsen over time, unless steps are taken now to address the problem.
Pressure on New Brunswick Emergency Departments
The Auditor General of New Brunswick analyzed data for 1,464,557 emergency department visits. They found that 66% of these visits did not meet the established CTAS targets for wait time from triage to physician assessment.
According to the Auditor General, there appear to be insufficient treatment spaces. Between April 1, 2020 and December 31, 2024, the percentage of treatment spaces available for emergency cases declined by 20 percentage points at Horizon and seven percentage points at Vitalité.[11]
The NBMS recommends that the Department of Health develop a comprehensive strategy to address emergency department needs including expected outcomes, benchmarks, timelines and resources required. The NBMS also recommends that the Department of Health monitor and report on the achievement of strategy results.
Relevant Legislation
New Brunswick Nursing Homes Act 2014, c.125 – Nursing Homes Act
General Regulation 85-187.pdf
References
Canadian Institute for Health Information (CIHI). (n.d.). Definitions and guidelines to support ALC designation in acute inpatient care. Retrieved from https://www.cihi.ca
Canadian Journal of Health Technologies. (2025). Alternate level of care in Canada: Evidence assessment report. Retrieved from https://cadth.ca
New Brunswick Health Council. (n.d.). Alternate level of care (ALC) hospitalizations. Retrieved from https://nbhc.ca
New Brunswick Health Council. (n.d.). Patient days in alternate level of care (ALC). Retrieved from https://nbhc.ca
New Brunswick Seniors’ Advocate. (2025). What we all want: Recommendation monitoring report. Retrieved from https://www.defenseur-nb-advocate.ca/resource/what-we-all-want%3A-recommendation-monitoring-report
New Brunswick Seniors’ Advocate. (2025). What we all want. Retrieved from https://www.defenseur-nb-advocate.ca/resource/what-we-all-want
Office of the Auditor General of New Brunswick. (2025). Report on emergency department performance. Retrieved from https://www.agnb-vgnb.ca/uploads/volume_translations/81/report/agnb-V2-2025-Report_E.pdf
CIHI. (2021). How many long-term care beds are there in Canada? Retrieved from https://www.cihi.ca/en/how-many-long-term-care-beds-are-there-in-canada
History
Approved by the New Brunswick Medical Society Board January 30, 2026.
[1] Canadian Institute for Health Information (CIHI) Definitions and Guidelines to Support ALC Designation in Acute Inpatient Care
[2] Canadian Journal of Health Technologies Alternate Level of Care in Canada: Evidence Assessment Report
[3] New Brunswick Health Council: Alternate Level of Care (ALC) hospitalizations | New Brunswick Health Council
[3] New Brunswick Health Council: Patient days in Alternate Level of Care (ALC) | New Brunswick Health Council
[4] New Brunswick Health Council: Alternate Level of Care (ALC) hospitalizations | New Brunswick Health Council
[5] New Brunswick Health Council: Patient days in Alternate Level of Care (ALC) | New Brunswick Health Council
[6] How many long-term care beds are there in Canada? | CIHI
[7] How many long-term care beds are there in Canada? | CIHI
[8] https://dfb1dee3-d35e-4ad0-84cb-92feb3cb37d1.filesusr.com/ugd/809eb9_ae40d2de80f84d73881c1ed2495be212.pdf
[9] Patient Days in Alternate Level of Care (Percentage) | CIHI
[10] Patient Days in Alternate Level of Care (Percentage) | CIHI
[11] agnb-V2-2025-Report_E.pdf
Contact
Jamie Yeamans, Policy and Economics Specialist, New Brunswick Medical Society at jyeamans@nbms.nb.ca